Exercise 7 Review Sheet Introduction to the Skeletal System and the Axial Skeleton
Bones are an of import role of the musculoskeletal system. This commodity, the first in a two-part serial on the skeletal system, reviews the anatomy and physiology of bone
Abstract
The skeletal organization is formed of basic and cartilage, which are continued by ligaments to form a framework for the rest of the body tissues. This commodity, the first in a two-part series on the structure and function of the skeletal arrangement, reviews the beefcake and physiology of os. Understanding the construction and purpose of the os allows nurses to empathise common pathophysiology and consider the most-appropriate steps to ameliorate musculoskeletal health.
Commendation: Walker J (2020) Skeletal system 1: the anatomy and physiology of bones. Nursing Times [online]; 116: 2, 38-42.
Writer: Jennie Walker is principal lecturer, Nottingham Trent University.
- This commodity has been double-bullheaded peer reviewed
- Scroll downward to read the commodity or download a print-friendly PDF hither (if the PDF fails to fully download please effort once again using a dissimilar browser)
- Read part 2 of this serial here
Introduction
The skeletal organization is composed of bones and cartilage connected past ligaments to form a framework for the residual of the body tissues. There are 2 parts to the skeleton:
- Axial skeleton – bones forth the axis of the body, including the skull, vertebral column and ribcage;
- Appendicular skeleton – appendages, such as the upper and lower limbs, pelvic girdle and shoulder girdle.
Function
Equally well as contributing to the body's overall shape, the skeletal system has several cardinal functions, including:
- Support and movement;
- Protection;
- Mineral homeostasis;
- Blood-cell formation;
- Triglyceride storage.
Support and movement
Basic are a site of attachment for ligaments and tendons, providing a skeletal framework that tin produce movement through the coordinated utilise of levers, muscles, tendons and ligaments. The bones human activity as levers, while the muscles generate the forces responsible for moving the bones.
Protection
Bones provide protective boundaries for soft organs: the attic effectually the encephalon, the vertebral column surrounding the spinal cord, the ribcage containing the heart and lungs, and the pelvis protecting the urogenital organs.
Mineral homoeostasis
As the primary reservoirs for minerals in the body, basic contain approximately 99% of the trunk'due south calcium, 85% of its phosphate and 50% of its magnesium (Bartl and Bartl, 2017). They are essential in maintaining homoeostasis of minerals in the blood with minerals stored in the bone are released in response to the body'south demands, with levels maintained and regulated by hormones, such as parathyroid hormone.
Blood-jail cell formation (haemopoiesis)
Blood cells are formed from haemopoietic stalk cells present in red bone marrow. Babies are born with only ruby bone marrow; over time this is replaced by yellow marrow due to a decrease in erythropoietin, the hormone responsible for stimulating the product of erythrocytes (cherry-red blood cells) in the bone marrow. By machismo, the amount of cerise marrow has halved, and this reduces further to around thirty% in older age (Robson and Syndercombe Court, 2018).
Triglyceride storage
Yellow bone marrow (Fig one) acts as a potential energy reserve for the body; it consists largely of adipose cells, which store triglycerides (a type of lipid that occurs naturally in the blood) (Tortora and Derrickson, 2009).

Bone composition
Bone matrix has three chief components:
- 25% organic matrix (osteoid);
- 50% inorganic mineral content (mineral salts);
- 25% water (Robson and Syndercombe Court, 2018).
Organic matrix (osteoid) is made up of approximately 90% blazon-I collagen fibres and 10% other proteins, such as glycoprotein, osteocalcin, and proteoglycans (Bartl and Bartl, 2017). It forms the framework for bones, which are hardened through the deposit of the calcium and other minerals around the fibres (Robson and Syndercombe Court, 2018).
Mineral salts are first deposited between the gaps in the collagen layers with in one case these spaces are filled, minerals accumulate around the collagen fibres, crystallising and causing the tissue to harden; this process is called ossification (Tortora and Derrickson, 2009). The hardness of the bone depends on the type and quantity of the minerals available for the body to utilize; hydroxyapatite is one of the chief minerals nowadays in basic.
While bones demand sufficient minerals to strengthen them, they too need to prevent being broken by maintaining sufficient flexibility to withstand the daily forces exerted on them. This flexibility and tensile strength of bone is derived from the collagen fibres. Over-mineralisation of the fibres or dumb collagen production tin can increase the brittleness of basic – as with the genetic disorder osteogenesis imperfecta – and increase bone fragility (Ralston and McInnes, 2014).
Structure
Os architecture is made up of two types of bone tissue:
- Cortical bone;
- Cancellous os.
Cortical bone
As well known equally compact bone, this dense outer layer provides support and protection for the inner cancellous construction. Cortical bone comprises iii elements:
- Periosteum (Fig i);
- Intracortical area;
- Endosteum (Bartl and Bartl, 2017).
The periosteum is a tough, fibrous outer membrane. It is highly vascular and almost completely covers the bone, except for the surfaces that form joints; these are covered by hyaline cartilage. Tendons and ligaments attach to the outer layer of the periosteum, whereas the inner layer contains osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells) responsible for bone remodelling.
The part of the periosteum is to:
- Protect the os;
- Assistance with fracture repair;
- Nourish bone tissue (Robson and Syndercombe Court, 2018).
Information technology also contains Volkmann's canals, small-scale channels running perpendicular to the diaphysis of the os (Fig ane); these convey blood vessels, lymph vessels and fretfulness from the periosteal surface through to the intracortical layer. The periosteum has numerous sensory fibres, so os injuries (such equally fractures or tumours) can exist extremely painful (Drake et al, 2019).
The intracortical os is organised into structural units, referred to as osteons or Haversian systems (Fig 2). These are cylindrical structures, composed of concentric layers of bone called lamellae, whose construction contributes to the strength of the cortical bone. Osteocytes (mature bone cells) sit down in the small-scale spaces betwixt the concentric layers of lamellae, which are known as lacunae. Canaliculi are microscopic canals between the lacunae, in which the osteocytes are networked to each other by filamentous extensions. In the centre of each osteon is a central (Haversian) culvert through which the blood vessels, lymph vessels and nerves pass. These primal canals tend to run parallel to the centrality of the bone; Volkmann's canals connect adjacent osteons and the blood vessels of the central canals with the periosteum.

The endosteum consists of a thin layer of connective tissue that lines the inside of the cortical surface (Bartl and Bartl, 2017) (Fig i).
Cancellous bone
Also known every bit spongy bone, cancellous bone is plant in the outer cortical layer. It is formed of lamellae arranged in an irregular lattice construction of trabeculae, which gives a honeycomb appearance. The large gaps between the trabeculae assist brand the bones lighter, and so easier to mobilise.
Trabeculae are characteristically oriented along the lines of stress to help resist forces and reduce the risk of fracture (Tortora and Derrickson, 2009). The closer the trabecular structures are spaced, the greater the stability and structure of the bone (Bartl and Bartl, 2017). Red or yellow os marrow exists in these spaces (Robson and Syndercombe Court, 2018). Crimson bone marrow in adults is establish in the ribs, sternum, vertebrae and ends of long basic (Tortora and Derrickson, 2009); information technology is haemopoietic tissue, which produces erythrocytes, leucocytes (white blood cells) and platelets.
Blood supply
Os and marrow are highly vascularised and account for approximately 10-20% of cardiac output (Bartl and Bartl, 2017). Blood vessels in bone are necessary for nearly all skeletal functions, including the delivery of oxygen and nutrients, homoeostasis and repair (Tomlinson and Silva, 2013). The claret supply in long bones is derived from the nutrient artery and the periosteal, epiphyseal and metaphyseal arteries (Iyer, 2019).
Each artery is also accompanied by nerve fibres, which branch into the marrow cavities. Arteries are the main source of blood and nutrients for long bones, entering through the nutrient foramen, then dividing into ascending and descending branches. The ends of long basic are supplied by the metaphyseal and epiphyseal arteries, which ascend from the arteries from the associated joint (Bartl and Bartl, 2017).
If the blood supply to bone is disrupted, it can result in the decease of os tissue (osteonecrosis). A common example is post-obit a fracture to the femoral neck, which disrupts the blood supply to the femoral head and causes the bone tissue to become necrotic. The femoral head structure then collapses, causing pain and dysfunction.
Growth
Bones brainstorm to class in utero in the start eight weeks post-obit fertilisation (Moini, 2019). The embryonic skeleton is first formed of mesenchyme (connective tissue) structures; this primitive skeleton is referred to as the skeletal template. These structures are then adult into bone, either through intramembranous ossification or endochondral ossification (replacing cartilage with bone).
Bones are classified according to their shape (Box ane). Flat bones develop from membrane (membrane models) and sesamoid bones from tendon (tendon models) (Waugh and Grant, 2018). The term intra-membranous ossification describes the direct conversion of mesenchyme structures to bone, in which the fibrous tissues become ossified every bit the mesenchymal stem cells differentiate into osteoblasts. The osteoblasts then start to lay down bone matrix, which becomes ossified to form new bone.
Box ane. Types of bones
Long bones – typically longer than they are wide (such as humerus, radius, tibia, femur), they comprise a diaphysis (shaft) and epiphyses at the distal and proximal ends, joining at the metaphysis. In growing bone, this is the site where growth occurs and is known as the epiphyseal growth plate. Near long bones are located in the appendicular skeleton and role equally levers to produce movement
Curt bones – small and roughly cube-shaped, these contain mainly cancellous bone, with a thin outer layer of cortical os (such equally the bones in the hands and tarsal bones in the feet)
Flat basic – thin and usually slightly curved, typically containing a sparse layer of cancellous bone surrounded by cortical bone (examples include the skull, ribs and scapula). Most are located in the axial skeleton and offering protection to underlying structures
Irregular basic – bones that practice non fit in other categories considering they accept a range of different characteristics. They are formed of cancellous bone, with an outer layer of cortical os (for example, the vertebrae and the pelvis)
Sesamoid bones – round or oval basic (such equally the patella), which develop in tendons
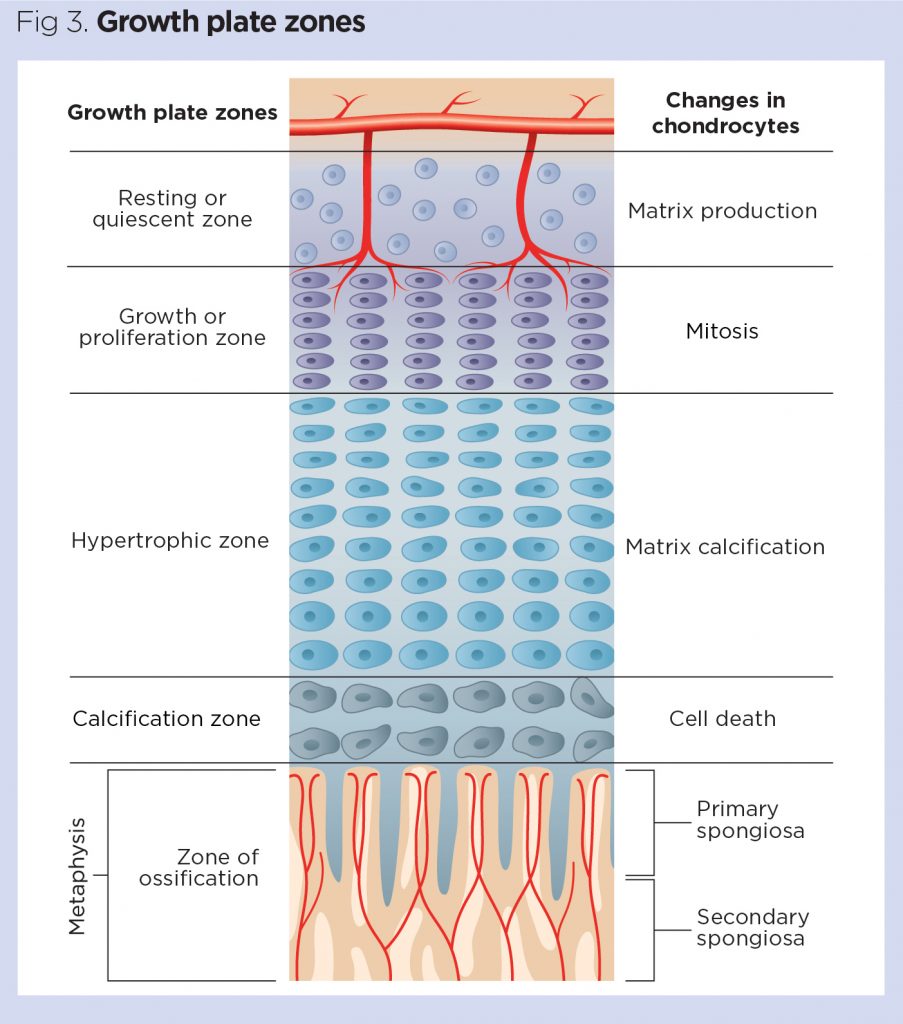
Long, brusk and irregular bones develop from an initial model of hyaline cartilage (cartilage models). In one case the cartilage model has been formed, the osteoblasts gradually replace the cartilage with os matrix through endochondral ossification (Robson and Syndercombe Court, 2018). Mineralisation starts at the centre of the cartilage structure, which is known as the master ossification centre. Secondary ossification centres also course at the epiphyses (epiphyseal growth plates) (Danning, 2019). The epiphyseal growth plate is composed of hyaline cartilage and has 4 regions (Fig 3):
Resting or quiescent zone – situated closest to the epiphysis, this is composed of small scattered chondrocytes with a depression proliferation charge per unit and anchors the growth plate to the epiphysis;
Growth or proliferation zone – this area has larger chondrocytes, arranged like stacks of coins, which carve up and are responsible for the longitudinal growth of the bone;
Hypertrophic zone – this consists of big maturing chondrocytes, which drift towards the metaphysis. At that place is no new growth at this layer;
Calcification zone – this final zone of the growth plate is only a few cells thick. Through the process of endochondral ossification, the cells in this zone become ossified and form office of the 'new diaphysis' (Tortora and Derrickson, 2009).
Bones are non fully developed at nascency, and continue to course until skeletal maturity is reached. By the end of adolescence around 90% of adult bone is formed and skeletal maturity occurs at around 20-25 years, although this tin can vary depending on geographical location and socio-economical conditions; for case, malnutrition may delay bone maturity (Drake et al, 2019; Bartl and Bartl, 2017). In rare cases, a genetic mutation can disrupt cartilage development, and therefore the development of os. This tin event in reduced growth and short stature and is known as achondroplasia.
The human growth hormone (somatotropin) is the chief stimulus for growth at the epiphyseal growth plates. During puberty, levels of sex activity hormones (oestrogen and testosterone) increase, which stops prison cell division within the growth plate. As the chondrocytes in the proliferation zone terminate dividing, the growth plate thins and eventually calcifies, and longitudinal os growth stops (Ralston and McInnes, 2014). Males are on average taller than females because male person puberty tends to occur later, so male bones take more time to grow (Waugh and Grant, 2018). Over-secretion of human growth hormone during childhood tin can produce gigantism, whereby the person is taller and heavier than normally expected, while over-secretion in adults results in a condition chosen acromegaly.
If there is a fracture in the epiphyseal growth plate while basic are even so growing, this tin subsequently inhibit os growth, resulting in reduced os germination and the os being shorter. It may also cause misalignment of the articulation surfaces and cause a predisposition to developing secondary arthritis later in life. A discrepancy in leg length can lead to pelvic obliquity, with subsequent scoliosis caused by trying to compensate for the difference.
Remodelling
Once bone has formed and matured, it undergoes constant remodelling past osteoclasts and osteoblasts, whereby one-time os tissue is replaced by new bone tissue (Fig four). Bone remodelling has several functions, including mobilisation of calcium and other minerals from the skeletal tissue to maintain serum homoeostasis, replacing onetime tissue and repairing damaged bone, as well every bit helping the torso conform to different forces, loads and stress applied to the skeleton.
Calcium plays a significant role in the body and is required for muscle contraction, nervus conduction, cell division and blood coagulation. As only one% of the body's calcium is in the blood, the skeleton acts as storage facility, releasing calcium in response to the body'south demands. Serum calcium levels are tightly regulated past 2 hormones, which piece of work antagonistically to maintain homoeostasis. Calcitonin facilitates the deposition of calcium to bone, lowering the serum levels, whereas the parathyroid hormone stimulates the release of calcium from bone, raising the serum calcium levels.
Osteoclasts are large multinucleated cells typically found at sites where there is agile bone growth, repair or remodelling, such as around the periosteum, inside the endosteum and in the removal of calluses formed during fracture healing (Waugh and Grant, 2018). The osteoclast cell membrane has numerous folds that face the surface of the os and osteoclasts break down bone tissue past secreting lysosomal enzymes and acids into the space betwixt the ruffled membrane (Robson and Syndercombe Court, 2018). These enzymes deliquesce the minerals and some of the bone matrix. The minerals are released from the bone matrix into the extracellular infinite and the balance of the matrix is phagocytosed and metabolised in the cytoplasm of the osteoclasts (Bartl and Bartl, 2017). In one case the expanse of bone has been resorbed, the osteoclasts motion on, while the osteoblasts motion in to rebuild the bone matrix.
Osteoblasts synthesise collagen fibres and other organic components that brand up the bone matrix. They as well secrete alkaline phosphatase, which initiates calcification through the deposit of calcium and other minerals around the matrix (Robson and Syndercombe Courtroom, 2018). As the osteoblasts deposit new bone tissue effectually themselves, they become trapped in pockets of bone called lacunae. In one case this happens, the cells differentiate into osteocytes, which are mature os cells that no longer secrete bone matrix.
The remodelling process is achieved through the balanced activity of osteoclasts and osteoblasts. If bone is built without the advisable balance of osteocytes, it results in abnormally thick bone or bony spurs. Conversely, too much tissue loss or calcium depletion can atomic number 82 to frail os that is more than susceptible to fracture. The larger surface area of cancellous bones is associated with a higher remodelling rate than cortical bone (Bartl and Bartl, 2017), which ways osteoporosis is more evident in basic with a high proportion of cancellous bone, such equally the caput/neck of femur or vertebral basic (Robson and Syndercombe Court, 2018). Changes in the remodelling remainder may also occur due to pathological conditions, such as Paget's affliction of bone, a condition characterised by focal areas of increased and disorganised os remodelling affecting 1 or more than basic. Typical features on X-ray include focal patches of lysis or sclerosis, cortical thickening, disorganised trabeculae and trabecular thickening.
As the torso ages, bone may lose some of its force and elasticity, making it more than susceptible to fracture. This is due to the loss of mineral in the matrix and a reduction in the flexibility of the collagen.
Diet and lifestyle factors
Adequate intake of vitamins and minerals is essential for optimum bone formation and ongoing bone wellness. Ii of the well-nigh important are calcium and vitamin D, but many others are needed to keep bones potent and salubrious (Box 2).
Box 2. Vitamins and minerals needed for os health
Key nutritional requirements for bone health include minerals such as calcium and phosphorus, besides equally smaller qualities of fluoride, manganese, and iron (Robson and Syndercombe Court, 2018). Calcium, phosphorus and vitamin D are essential for effective bone mineralisation. Vitamin D promotes calcium absorption in the intestines, and deficiency in calcium or vitamin D tin can predispose an individual to ineffective mineralisation and increased risk of developing conditions such as osteoporosis and osteomalacia.
Other cardinal vitamins for healthy bones include vitamin A for osteoblast function and vitamin C for collagen synthesis (Waugh and Grant, 2018).
Physical exercise, in particular weight-bearing do, is important in maintaining or increasing bone mineral density and the overall quality and strength of the bone. This is because osteoblasts are stimulated by load-begetting exercise and and then bones subjected to mechanical stresses undergo a higher rate of bone remodelling. Reduced skeletal loading is associated with an increased hazard of developing osteoporosis (Robson and Syndercombe Court, 2018).
Conclusion
Bones are an important part of the musculoskeletal system and serve many core functions, likewise as supporting the trunk's structure and facilitating movement. Bone is a dynamic construction, which is continually remodelled in response to stresses placed on the body. Changes to this remodelling process, or inadequate intake of nutrients, can issue in changes to bone structure that may predispose the body to increased risk of fracture. Part 2 of this series will review the structure and function of the skeletal system.
Key points
- Bones are key to providing the torso with structural support and enabling motility
- Most of the trunk'south minerals are stored in the bones
- Nutrition and lifestyle tin touch the quality of os formation
- Later bones take formed they undergo abiding remodelling
- Changes in the remodelling process can result in pathology such every bit Paget's disease of os or osteoporosis
References
Bartl R, Bartl C (2017) Construction and architecture of bone. In: Os Disorder: Biology, Diagnosis, Prevention, Therapy.
Danning CL (2019) Construction and part of the musculoskeletal arrangement. In: Banasik JL, Copstead Fifty-EC (eds) Pathophysiology. St Louis, MO: Elsevier.
Drake RL et al (eds) (2019) Greyness'south Anatomy for Students. London: Elsevier.
Iyer KM (2019) Anatomy of os, fracture, and fracture healing. In: Iyer KM, Khan WS (eds) General Principles of Orthopedics and Trauma. London: Springer.
Moini J (2019) Bone tissues and the skeletal system. In: Anatomy and Physiology for Health Professionals. Burlington, MA: Jones and Bartlett.
Ralston SH, McInnes IB (2014) Rheumatology and bone disease. In: Walker BR et al (eds) Davidson's Principles and Practice of Medicine. Edinburgh: Churchill Livingstone.
Robson 50, Syndercombe Court D (2018) Bone, musculus, skin and connective tissue. In: Naish J, Syndercombe Court D (eds) Medical Sciences. London: Elsevier
Tomlinson RE, Silva MJ (2013) Skeletal claret flow in bone repair and maintenance. Bone Research; one: four, 311-322.
Tortora GJ, Derrickson B (2009) The skeletal system: bone tissue. In: Principles of Anatomy and Physiology. Chichester: John Wiley & Sons.
Waugh A, Grant A (2018) The musculoskeletal system. In: Ross & Wilson Anatomy and Physiology in Wellness and Illness. London: Elsevier.
Source: https://www.nursingtimes.net/clinical-archive/orthopaedics/skeletal-system-1-the-anatomy-and-physiology-of-bones-27-01-2020/
0 Response to "Exercise 7 Review Sheet Introduction to the Skeletal System and the Axial Skeleton"
Post a Comment